
Imagine waking up every morning feeling truly rested, without the hum of a machine or the discomfort of a mask strapped to your face. For millions of people suffering from obstructive sleep apnea (OSA), this sounds like a fantasy. If you have tried continuous positive airway pressure (CPAP) therapy and found it unbearable-whether due to claustrophobia, dry mouth, or simple irritation-you are not alone. Abandonment rates for CPAP hover between 29% and 46%, leaving many patients untreated and at risk for serious health complications. But there is another path forward that doesn't involve masks or hoses.
This path is called upper airway stimulation, an FDA-approved implantable therapy designed specifically for moderate to severe OSA patients who cannot tolerate CPAP. It works by gently stimulating the nerve that controls your tongue, keeping your airway open while you sleep naturally. In this guide, we will break down how this technology works, who qualifies for it, what the surgery entails, and whether it might be the right solution for you.
How Upper Airway Stimulation Works
To understand upper airway stimulation, you first need to understand why sleep apnea happens. In most cases of obstructive sleep apnea, the muscles in your throat relax too much during sleep, causing your tongue and soft tissues to collapse into your airway. This blockage stops airflow, leading to gasping, snoring, and fragmented sleep.
Inspire Upper Airway Stimulation is an implantable medical device developed by Inspire Medical Systems that treats obstructive sleep apnea by delivering mild electrical pulses to the hypoglossal nerve. The hypoglossal nerve is the command center for your tongue. When stimulated, it causes your tongue to move slightly forward, pulling the airway open just enough to allow air to flow freely.
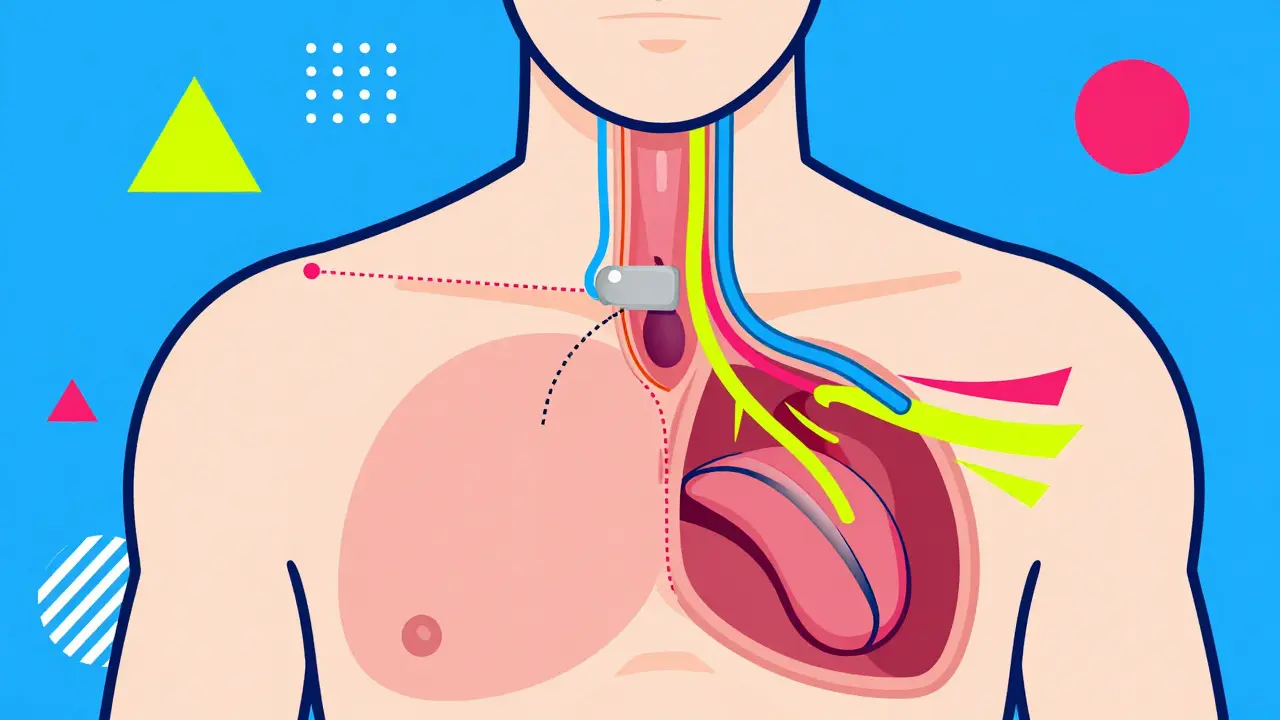
The system consists of three parts implanted inside your body:
- An implantable pulse generator (IPG), similar in size to a pacemaker, placed under the skin in your chest.
- A sensing lead placed on your diaphragm to detect when you inhale.
- A stimulation lead attached to the hypoglossal nerve in your neck.
Before bed, you use a small remote control to turn the device on. As you breathe in, the sensor detects the movement and sends a mild signal to the nerve, opening your airway. When you exhale, the stimulation pauses. This cycle repeats throughout the night, synchronized perfectly with your natural breathing pattern. You don't feel the stimulation; it’s subtle and painless. Most users report that they simply wake up feeling more alert and less tired than they have in years.
Who Is a Candidate for UAS Therapy?
Not everyone with sleep apnea is a good candidate for upper airway stimulation. Because this is a surgical procedure, doctors follow strict criteria to ensure safety and effectiveness. The American Academy of Sleep Medicine (AASM) and the FDA have outlined specific guidelines that must be met before you can proceed.
Generally, you may qualify if you meet all of the following conditions:
- You have been diagnosed with moderate to severe obstructive sleep apnea, defined as an Apnea-Hypopnea Index (AHI) between 15 and 100 events per hour.
- You have tried CPAP therapy for at least three months and failed to adhere to it consistently (using it fewer than four hours per night on less than 70% of nights).
- Your Body Mass Index (BMI) is less than 35 kg/m². Note that in 2023, the FDA expanded approval to include patients with a BMI up to 40 kg/m², broadening eligibility significantly.
- You do not have complete concentric collapse of the soft palate. This is determined through a drug-induced sleep endoscopy (DISE) test.
- You are at least 22 years old.
- You have less than 25% central or mixed apneas, meaning your apnea is primarily caused by physical obstruction rather than brain signaling issues.
If you fall outside these ranges-for example, if you have significant central sleep apnea or a BMI over 40-you might still benefit from other treatments like oral appliances or traditional surgery. Your sleep specialist will perform a detailed evaluation to determine the best option for your anatomy.
The Surgery and Recovery Process
One of the biggest concerns patients have is the idea of surgery. While upper airway stimulation does require an operation, it is minimally invasive and performed on an outpatient basis. You go home the same day.
The procedure typically takes two to three hours under general anesthesia. Surgeons make three small incisions:
- One in the upper neck to access the hypoglossal nerve.
- One in the lower neck to place the pressure sensor.
- One below the collarbone to insert the pulse generator.
After surgery, you’ll spend a few days recovering at home. Most people return to normal activities within five to seven days. You won’t be able to activate the device immediately. It takes about four weeks for the surgical sites to heal completely. During this time, you’ll continue using CPAP or another temporary method to manage your apnea.
Once healing is complete, you’ll visit your doctor for activation. They will program the device to match your breathing patterns and teach you how to use the remote. Follow-up appointments usually occur at one, three, six, and twelve months to fine-tune the settings and monitor progress.
Effectiveness and Real-World Results
Does upper airway stimulation actually work? Clinical trials and real-world data say yes. The landmark STAR trial (Stimulation Therapy for Apnea Reduction) followed patients for 12 months and found that the average AHI dropped from 29.3 events per hour to just 9.0-a 68% reduction. More importantly, 66% of participants achieved both a greater than 50% reduction in AHI and an AHI below 20, which is considered clinically successful.
Long-term studies like the ADHERE Registry show consistent results even in patients with higher BMIs and more severe disease. Patients reported significant improvements in daytime sleepiness, energy levels, and overall quality of life. Bed partners also noticed changes: 85% reported no snoring or only soft snoring after four years of use.
Adherence is where UAS really shines. Unlike CPAP, which requires nightly commitment to wearing a mask, UAS has usage rates exceeding 80%. Why? Because once the device is activated, it works automatically. There’s no mask to adjust, no hose to tangle, and no claustrophobia. For many, this simplicity makes all the difference.
| Treatment | Invasiveness | Adherence Rate | Best For | Reversibility |
|---|---|---|---|---|
| CPAP | Non-invasive | 54-71% | All severities | N/A |
| Upper Airway Stimulation | Surgical implant | >80% | Moderate-severe OSA, CPAP intolerant | Yes (device removal) |
| Oral Appliances | Non-invasive | ~70% | Mild-moderate OSA | Yes |
| UPPP Surgery | Major surgery | N/A | Specific anatomical blocks | No |
Costs and Insurance Coverage
Cost is often a major concern when considering any medical procedure. Upper airway stimulation is expensive upfront. The total cost-including the device, surgeon fees, hospital stay, and follow-ups-typically ranges from $35,000 to $40,000. However, this is comparable to the long-term cost of CPAP when you factor in equipment replacements, filters, masks, and ongoing care over several years.
The good news is coverage has improved dramatically. As of 2026, 95% of Medicare beneficiaries and 85% of commercially insured patients in the U.S. have coverage for UAS therapy. Many insurance plans now recognize it as a standard treatment for eligible patients. Before proceeding, ask your provider to submit a pre-authorization request to confirm your benefits.
If you’re paying out-of-pocket, some manufacturers offer financing options or payment plans. Always check with your local healthcare providers for current pricing and assistance programs.

Potential Risks and Side Effects
Like any surgery, upper airway stimulation carries risks. Fortunately, serious complications are rare. According to real-world data, the major complication-free rate is 99.6%. Minor side effects may include:
- Temporary tongue weakness or numbness (reported in about 5% of patients).
- Surgical site infection (around 2%).
- Pain or discomfort at the incision sites during recovery.
Most side effects resolve within weeks. Serious adverse events occur in less than 0.5% of cases. The device itself is safe and well-tested, with over 200,000 implants performed worldwide since its initial approval in 2014.
It’s important to remember that UAS is not a cure for sleep apnea-it’s a management tool. You still need to maintain healthy habits, such as losing weight if overweight, avoiding alcohol before bed, and sleeping on your side. These lifestyle changes can enhance the effectiveness of the therapy.
Living with the Device
Once fully healed and activated, living with upper airway stimulation is surprisingly simple. Each night, you press a button on your remote to turn the device on. That’s it. No adjustments needed unless your doctor recommends titration changes during follow-ups.
Some users forget to activate the device occasionally. To help build the habit, try placing the remote next to your phone charger or alarm clock. Others worry about magnet interference. The device is shielded against common household magnets, but avoid strong magnetic fields like MRI machines unless cleared by your doctor.
Traveling is easy-the device stays with you. Just pack your remote and any charging cables. International travelers should carry their medical documentation in case questions arise at customs or airports.
When to Consider Alternatives
Upper airway stimulation isn’t for everyone. If you have mild sleep apnea, oral appliances might be sufficient. If you prefer non-surgical options and can tolerate CPAP, stick with it-it remains the gold standard for efficacy across all severities. Traditional surgeries like uvulopalatopharyngoplasty (UPPP) may be considered if you have specific structural abnormalities that don’t respond to other treatments.
Talk openly with your sleep specialist about your preferences, lifestyle, and goals. They can help you weigh the pros and cons of each approach based on your unique situation.
Is upper airway stimulation painful?
The surgery involves general anesthesia, so you won’t feel anything during the procedure. Afterward, you may experience mild soreness or swelling for a few days, manageable with prescribed pain medication. The stimulation itself is not felt during sleep.
Can I remove the device later?
Yes, upper airway stimulation is reversible. If you choose to stop treatment, a surgeon can remove the implant components through a minor procedure. This is different from permanent surgeries like UPPP.
How long does the battery last?
The implantable pulse generator battery lasts approximately 10 years. Replacement requires another outpatient surgery, but the process is straightforward and widely performed.
Does insurance cover upper airway stimulation?
Coverage varies by plan, but as of 2026, most major insurers including Medicare cover UAS for eligible patients. Check with your provider and insurer for pre-authorization requirements.
What happens if I forget to turn on the device?
If you forget to activate the device, you’ll likely experience typical sleep apnea symptoms that night. There’s no penalty or damage to the device. Simply remind yourself to use the remote each night as part of your bedtime routine.


May 11, 2026 AT 03:14 AM
I have been following the clinical data on upper airway stimulation for several years, and the results are genuinely impressive when you look past the marketing hype. The key is understanding that this is not a magic bullet but a sophisticated neuromodulation therapy.
The mechanism relies on precise synchronization with respiration, which requires a healthy diaphragm signal. This is why the screening process is so rigorous. Many patients assume they qualify because they hate CPAP, but the anatomical requirements are strict. You need a specific type of collapse-lingual or palatal-that responds to tongue advancement.
If you have concentric collapse at the level of the soft palate, stimulating the hypoglossal nerve won't help because the blockage is higher up. That's why the Drug-Induced Sleep Endoscopy (DISE) is non-negotiable. It maps your unique airway anatomy while you're under sedation.
Also, consider the long-term maintenance. While adherence is higher than CPAP, you still need to remember to turn it on. For some, this is easier than donning a mask; for others, it's another step in the bedtime routine. But the quality of life improvement reported by users who succeed is profound. They wake up refreshed, their partners stop complaining about snoring, and the cardiovascular risks associated with untreated OSA begin to decline. It’s a significant investment in health, both financially and physically.
May 11, 2026 AT 22:43 PM
they want you to believe it's safe but have you noticed how many of these 'studies' are funded by the device manufacturer? big medtech loves to bury the bad data. i read somewhere that the battery degradation can cause erratic firing patterns after year seven. nobody talks about that. they just want your $40k. think about it. why would they expand the bmi limit unless they needed more bodies to test on? it's all about shareholder value, not your sleep. stay awake, stay suspicious.
May 13, 2026 AT 17:22 PM
Look, I’m not here to debate the efficacy of the device itself, the data seems solid enough for those who qualify. What bothers me is the casual dismissal of CPAP intolerance as a simple preference issue. People don’t just 'not like' the mask; many have claustrophobia or facial injuries that make it physically impossible.
Saying 'just stick with it' is useless advice. If you’ve tried for six months and still can’t tolerate it, you’re not failing; the treatment is failing you. Upper airway stimulation offers a legitimate alternative for that specific demographic. However, we need to be realistic about the surgical risk. It’s minimally invasive, yes, but it’s still surgery. Infection, nerve damage, hardware failure-these aren't zero probabilities.
Don’t let anyone guilt-trip you into staying on a machine that ruins your nights. If you meet the criteria, explore UAS. But do your homework. Talk to surgeons who have done hundreds of these, not just one. And check your insurance pre-auth requirements before you even book the consult.
May 14, 2026 AT 23:14 PM
i used to think surgery was the last resort but maybe it is the first step for some people. the idea of waking up without thinking about breathing is appealing. i am curious about the remote control aspect though. does it feel weird having to press a button every night? or does it become automatic like brushing teeth. also what happens if you travel internationally. do you need special clearance at airports for the metal implant. i imagine security scanners might go crazy.
May 15, 2026 AT 00:35 AM
Hey @Dat Alexander! 👋 Great question about the airport security. Most users report that TSA doesn't flag the Inspire device specifically, but it’s always smart to carry your medical ID card.
As for the remote, it becomes muscle memory pretty quickly. Think of it like turning off your alarm clock. You press it, you sleep. It’s designed to be intuitive. The real win is the silence in the bedroom. My partner and I were skeptical at first, but the difference in our relationship dynamics since he got his device has been huge. No more waking up angry from snoring sounds. 🌟
May 16, 2026 AT 07:53 AM
u ppl r so naive!!! 😡 they say its safe but look at the side effects list carefully. tongue numbness?? that means nerve damage. permanent. u cant taste ur food properly anymore. and the infection rate is hidden in the fine print. i saw a post where a guy said his device migrated under his skin. painful right??? dont trust big pharma. keep ur money and use mouth guards instead. natural is better. 💅
May 17, 2026 AT 01:56 AM
The epistemological framework surrounding the promotion of upper airway stimulation is deeply flawed. We are witnessing a shift from evidence-based medicine to profit-driven interventionism. The claim that 'abandonment rates' justify surgical implants ignores the root causes of CPAP non-adherence, which are often socioeconomic or educational gaps rather than physiological intolerance.
To suggest that a patient should undergo an invasive procedure involving foreign body implantation simply because they find a mask uncomfortable is ethically questionable. The 'gold standard' remains CPAP for a reason: it is non-invasive and reversible. UAS introduces a dependency on proprietary technology with a finite lifespan. When the battery dies, you are back to square one, minus the cost of a replacement surgery.
We must scrutinize the long-term neurological effects of chronic hypoglossal nerve stimulation. Are we causing micro-trauma to the nerve endings over a decade of use? The data is insufficient. Until we have longitudinal studies spanning twenty years, promoting UAS as a 'solution' is premature and potentially harmful to public health literacy.
May 17, 2026 AT 19:03 PM
You are missing the point entirely, Mr. Fibelkorn!! The issue is not 'socioeconomic gaps'!! It is the sheer brutality of the CPAP machine!! Who wants to wear a plastic muzzle every night for the rest of their life?? It is dehumanizing!!! The implant restores dignity!! Yes, there are risks, but living in a fog of fatigue is worse!! You sound like a bot programmed to defend the status quo!! Wake up!! The nerve stimulation is gentle!! It is precise!! It is the future!! Why do you resist progress?? Are you afraid of change?? Or are you just jealous of people who can finally sleep through the night without humming noises?? 🤬🤬🤬
May 18, 2026 AT 11:50 AM
i mean sure if u have money its great but most of us dont. 40k is a lot. i tried cpap too and hated it but i couldnt afford the surgery. so i just bought a chin strap online and it helps a little bit. not perfect but better than nothing. why do doctors only push the expensive stuff. probably getting kickbacks. makes me mad that healthcare is so broken. just want to sleep peacefully lol.
May 19, 2026 AT 06:30 AM
This entire narrative is a triumph of American medical capitalism over common sense. We are told to fear the humble CPAP mask-a piece of plastic and rubber-and instead embrace a $40,000 electronic pacemaker for our tongues. It is absurd.
CPAP works. It has saved millions of lives. The fact that people complain about 'discomfort' is a testament to their fragility. If you cannot tolerate a mild airflow to keep your airway open, perhaps you should examine your own resilience.
Furthermore, the expansion of BMI criteria is a slippery slope. We are now operating on obese individuals who refuse to address the root cause of their apnea: weight. Inserting a device into a morbidly obese patient is a band-aid on a bullet wound. It delays the inevitable complications of obesity while enriching the shareholders of Inspire Medical Systems.
Let us not be seduced by the promise of 'mask-free' nights. The trade-off is surgical risk, hardware dependency, and financial ruin. Stick to the proven methods. Lose the weight. Wear the mask. Grow up.
May 20, 2026 AT 06:49 AM
@Brian LeClercq your tone is quite aggressive. while i agree that weight loss is important for overall health, dismissing CPAP intolerance as 'fragility' is not helpful. many people have genuine physical issues with masks. for them, uas is a valid option. we should support choices that improve quality of life without judgment. everyone's journey is different. peace 🕊️
May 20, 2026 AT 18:28 PM
Haha, Brian, you really went full villain mode there 😂. Look, I get the frustration, but let's be real. If CPAP worked for everyone, we wouldn't need alternatives. I know guys who literally gagged on the mask. They couldn't breathe through their noses either. So yeah, for them, the implant is a lifesaver. Not a 'capitalist trap', just a tool. Don't knock it until you've worn it for 8 hours straight. 🤷♂️
May 22, 2026 AT 06:58 AM
ive been reading all these comments and its interesting how divided people are. i had the surgery two years ago and honestly it changed my life. i was skeptical at first because of the cost and the recovery time. but once it kicked in, i stopped waking up gasping for air. my wife says i dont snore anymore which is huge for her. the only downside is the monthly visits to adjust settings but thats minor compared to sleeping well. if you qualify and insurance covers it, its worth considering. just make sure you do your research and talk to a specialist you trust. dont listen to haters.
May 23, 2026 AT 16:56 PM
Raymond, thank you so much for sharing your experience! It is incredibly reassuring to hear from someone who has actually gone through the process. I have been struggling with CPAP for years, and the thought of surgery always scared me. But hearing that you no longer wake up gasping gives me hope.
I am particularly interested in knowing more about the adjustment period. Did you miss work for a long time? And how did you manage the pain during the first few weeks? I am worried about being able to care for my kids during recovery. Any tips on making the home environment more comfortable would be greatly appreciated. Your story is truly inspiring! 💖